Parents As Teachers & Early Head Start
Every child should have the opportunity to reach their full potential.
Parents as First Teachers

At Kids’ Corps, we believe that parents are a child’s first and most important teacher. Our program is designed to provide parents with information and assistance to embrace their role as their child’s first teacher to enhance their child’s intellectual, language, social-emotional and physical development from birth to age five.
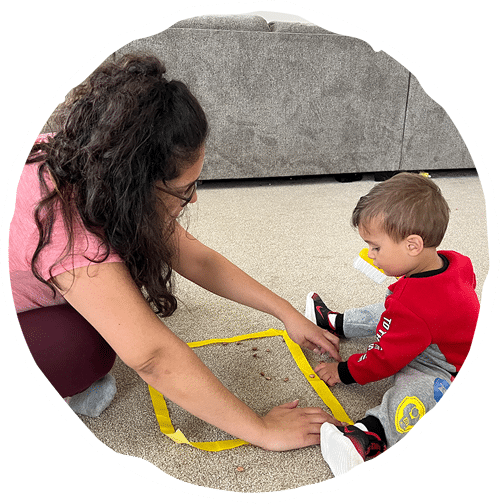
Our home visiting professionals meet families where they are comfortable, typically in their home. On each home visit a parent educator shares developmentally appropriate child development and parenting information for families to help them learn to observe their child and address any parenting concerns. Each visit includes:
- A fun parent/child activity designed to enrich parent/child interactions and enhance child development
- Discussion and handouts based on each child’s particular stage of development with information on fun activities to nurture growth
- An opportunity to receive research-based answers to parenting and child development questions

FAQ’S
Our parent educators meet families every other week where they are comfortable, typically in their home. During visits, parent educators assess family needs and partner with parents to set family goals. Home visitors provide necessary information and resources to help parents support the emotional, behavioral and physical development of their children. Each personal visit includes a focus on parent-child interaction, development-centered parenting and family well-being.
Each Visit Includes:
Activity
A fun parent/child activity provided is designed to enrich parent/child interactions and enhance child development.

Nurture
Discussion and handouts are based on each child’s particular stage of development with information on fun activities to nurture growth.

Education
An opportunity to receive research-based answers to parenting and child development questions.

Health
At parent’s request, children are screened for hearing, vision, health and developmental concerns. If additional help is required, the Parent Educator will provide referrals to services in the community and assist the family in connecting with the appropriate provider.
Families in the program are invited to participate in group connection activities that are hosted two times each month. These events give parents the opportunity to learn and share information on parenting issues and child development. Parents learn from and support each other, observe their children with other children, practice parenting skills and enjoy fun activities with their children and other families.
Topics For Group Connections Include:
Literacy
Nutrition
Music
Art
Learning begins at birth and research suggests that from birth to three years of age – and especially during the first six months of life – the brain goes through the most critical stage of development.
Learning Begins at Birth
By age 3
most children have learned 75% of all the language skills they will have as adults.
In the first years
children learn more and at a much faster pace than any other time in life.
A child’s brain
by age three is already 80% of the size of an adult brain.
Through The Program:

Achieve
Children achieve school success into the elementary grades.

Improve
Parents improve their parenting knowledge and skills.

Involved
Parents are more involved in their children’s schooling.
Promote
Families are more likely to promote children’s language and literacy.

Kids’ Corps, Inc. has become a massive part of our everyday lives… it has met my every need as a professional and parent.
Ariel-leu
Parent & Staff
PAT Highlights
KCI Blue Ribbon Affiliate Certificate
Through the successful completion of the Quality Endorsement and Improvement Process, Kids’ Corps, Inc. is hereby recognized as a Blue Ribbon Affiliate.
KCI PAT 2021-2022 Affiliate Report
PDF versions of the APR questions AND a detailed set of instructions are available on the APR Portal to assist with completion of the APR.
KCI PAT 2020 Essential Requirements Review
Performance Measures Report for Service Delivery Essential Requirements.








